Breast augmentation can be done in varied ways (e.g., incision placement, implant type, size, and positioning, combinations with other surgeries such as breast lifting). And when you remember that each woman is different, e.g. in the nature of her breast tissue, in her body’s reaction to the surgery, and in her expectations of the outcome – then you can see how many possible post-op scenarios there are. As many as there are women having breast augmentation surgery!
So in this short article, we’ll discuss possible complications in general terms, bearing in mind that almost all complications can be dealt with, at least to some extent, and that being well-informed before surgery and carefully cleaned and cared-for afterwards will prevent most complications. Of course, if you want some more hands-on consultation about breast augmentation, you might consider contacting a plastic surgeon.
INFECTION
This is a rare complication with any surgery and will occur in the first month or so post-op, if at all. You can help prevent it by washing your breasts with anti-bacterial soap for several days before surgery, and your armpits too, if you’re planning to have the transaxillary incision. Of course, the surgeon will swab these areas too, with Betadine. If you have the periareolar incision (around the areola), there’s a slightly greater chance of infection because bacteria may be in the milk ducts. The most obvious sign of infection will be a high fever. In rare cases, the implant may have to be removed and a waiting period will ensue, perhaps several months, before it can be re-inserted.
BOTTOMING OUT
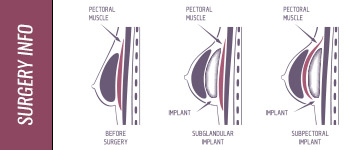
Sometimes an implant will shift to a lower position, leaving the nipple sitting up too high, and this will look unnatural. It might be caused by the pocket in which the implant nestles being too big, or by the woman’s skin and natural breast tissue being too scanty for the size of the implant. Some cosmetic surgeons claim the use of a strongly supportive bra immediately post-op for several weeks can prevent this complication. However, if it occurs, it will most likely require further surgery and re-suturing. It’s more likely to happen when the breast implants are placed sub-glandular, i.e., above the muscle. In this position, they have no support at their lower edge. When they’re placed under the muscle, and especially when they’re under the fascia as well, they have a strong natural support at their lower edge, formed by that muscle and fascia.
CAPSULE CONTRACTURE
After the breast implant has been in position for a few weeks or months, the body will naturally grow some fibrous tissue over it. Capsule contracture (or capsular contracture) refers to this fibrous tissue tightening around the implant, and squeezing it. Mild cases are not really complications, but severe cases cause pain and a hardening of the breast. Further surgery must be performed then, to scrape out this tissue and give the breast implant more space.
RIPPLING
After the post-op swelling subsides and the breast implant settles into its position, it pulls on that fibrous scar tissue described under Capsule contracture. This in turn pulls on the skin, causing wrinkling, or rippling. Cosmetic surgeons still debate the cause of this complication. Some say that use of a breast implant with a textured surface is what causes the rippling and that using a smooth breast implant instead will avoid it. Others say that on the contrary, using a textured implant will avoid it. And some say that it’s unrelated to the type of breast implant, but rather is related to incorrect filling of the implant after it’s in position. However, sub-muscular placement of the implant is thought to avoid most of it, since the implant is then separated from the skin by both muscle and breast tissue.
INTERFERENCE WITH MAMMOGRAMS
If the implant is placed sub-glandular, (above the muscle), whether it’s a saline or silicone gel breast implant, it can hide potentially cancerous tissue. Sub-muscular placement reduces this risk. The technician performing the mammogram should be informed of the implants, so appropriate techniques can be used. Usually, more views will have to be taken, even if the implants are sub-muscular.
RUPTURE
Any breast implant, in any placement, can at some point rupture, or tear, allowing the filling, whether saline solution or silicone gel, to leak into surrounding tissue. Simple wear and tear can eventually cause a rupture. No breast implant lasts for a lifetime. Working out with weights, a careless mammogram technician, improper filling of the implant, even the years of breathing, can all damage or weaken the implant’s shell and lead to rupture. If the implant is saline-filled, deflation will occur within several hours and you’ll know there’s been a rupture. If it’s a silicone-gel breast implant, months may go by before enough of the thick gel can leak out to catch your attention. When a rupture happens, the implant must be replaced.
HEMATOMA, SEROMA, THROMBOSIS
A hematoma is a pool of clotted blood under the skin and is a risk of any surgery. It may cause a painful lump but is correctible by surgery.
A seroma is a pool of fluid that sometimes collects around the implant. It is easily drained off with a needle.
A thrombosis is a blood clot that on rare occasions may form in a vein and interfere with blood circulation. Surgery can deal with it.
SYNMASTIA
Sometimes, if the cosmetic surgeon works on creating more cleavage, he may be too enthusiastic in cutting tissue over the sternum (breastbone). The implants may subsequently move closer together and actually touch, making the breasts join and eliminating cleavage. That movement of the implants can be started by the post-op bandages squeezing them in too much from the sides, or by sleeping on your side. Further surgery is necessary to correct it.
Some Very Rare Complications Are:
Galactorrhea: the implant stimulates breast milk (if this doesn’t cease spontaneously, the breast implants must be removed)
Necrosis: death of breast tissue (may happen after chemotherapy, or if excessive smoking has impaired blood circulation)
Extrusion: the body rejects the breast implants and tries to push them out (implants must be promptly removed, before the breast skin is broken)